1. Introduction
Endometrial cancers (ECs) are tumors of the inner part of the uterus, deriving mostly from the glandular tissue. ECs account for 75–80% of all uterine cancers, and represent one of the most common gynecologic malignancies, affecting ∼3% of women [
1]. The risk of EC development is associated with genetic predisposition (e.g., Lynch syndrome), racial background, age, obesity, metabolic syndrome, diabetes, polycystic ovary syndrome, and high estrogen exposure. Metabolic conditions related to lifestyle represent the most significant risk factors [
2,
3,
4,
5,
6,
7]. Currently, EC incidence and mortality are continuously rising, with the highest rates registered in North America and Europe [
8].
Based on epidemiological, clinical, pathological, and molecular characteristics, ECs are classified into two different subtypes. Type I ECs represent the majority of new cases, usually low-grade and associated with a favorable prognosis. Common features of type I ECs are endometrioid cell morphology resembling the normal endometrium (low-grade, I or II), and expression of estrogen receptors [
9,
10]. Type II ECs are more aggressive forms, usually hormone-receptor-negative high-grade tumors with poor prognoses. Histologically, type II ECs are mainly characterized by being serous and clear cell undifferentiated carcinomas and carcinosarcomas [
9,
10].
At clinical presentation, EC symptoms are poorly specific, which include abnormal uterine bleeding as the most common symptom in advanced stages in post-menopause women. In advanced EC, bleeding is often accompanied by abdominal and pelvic pain [
11]. Currently, there are no specific tests for the diagnosis of EC; standard diagnostic protocols consist of pelvic ultrasonography, and a certain diagnosis commonly requires invasive investigation procedures, such as hysteroscopy, with targeted biopsy or blinded dilation and curettage (D & C) [
12]. Expanding biological understanding of EC and refining its molecular characterization is still challenging, but such strategies may uncover new exploitable biomarkers. The use of proteomic techniques is making a great contribution to understanding the pathophysiology of tumors [
13]. Using proteomic methodologies allows us to identify putative biomarkers in different cancers, including gastric cancer [
14], liver cancer [
15], and ovarian cancer [
16]. In EC, numerous biomarkers have been reported from different biological samples (including tumor tissue, blood, serum, plasma, urine, and uterine lavage fluid), but none have reached the clinical stage thus far ([
17,
18], Njoku 2019). The identification of circulating biomarkers may allow for easy detection, avoiding invasive sampling procedures. Thanks to a proteomic study, we recently identified new putative biomarkers in the sera of EC patients (namely SBSN [
19], CLU, SERPINC1, ITIH4, C1R [
20], GAL-9, GAL-1, MMP7, FASLG, and COL9A1 [
21]).
A growing body of evidence has shown that tumor cells release a plethora of extracellular vesicles (EVs) that carry lipids, proteins, DNA, mRNAs, and miRNAs [
22]. Among them, the best characterized are exosomes, microvesicles that originate in the multivesicular body and measure 30–100 nm in diameter; they are released in body fluids, including blood, bile, urine, and saliva [
23]. From a clinical perspective, finding key mediators of EC released in exosomes may allow us to identify potential biomarkers of cancer development and progression. By applying LC-MS/MS, Song Y and colleagues recently identified LGALS3BP as a possible biomarker in the plasmatic exosome of EC [
24]. Here, using a label-free quantification (LFQ) proteomics approach, the present study aimed to characterize the exosomal proteome from the albumin-depleted serum, in order to identify novel EC biomarkers.
2. Materials and Methods
2.1. Patients
For proteomic and data validation, a total of 72 patients (36 women suffering from EC, and 36 non-EC controls) were recruited at the Institute for Maternal and Child Health—IRCCS “Burlo Garofolo” (Trieste, Italy) during 2019 and 2021. All procedures complied with the Declaration of Helsinki, and were approved by the Institutional Review Board of IRCCS Burlo Garofolo and the Regional Ethics Committee (CEUR-2020-Os-030). All patients signed informed consent forms. The clinical and pathological characteristics of the patients are described in
Supplementary Materials Table S1. The median age of the patients was 68 years (Interquartile Range: IQR 57–75; Min = 48, Max = 88), while the median age of the controls was 38 (IQR 28–54; Min = 23, Max = 78). Subjects who were positive to human immunodeficiency virus (HIV) or hepatitis B or C virus (HBV, HBC) were excluded from the study. The controls who were chosen excluded oncologic patients, and patients with leiomyomas or adenomyosis. In this study, we also excluded controls with benign tumors (myoma), chronic inflammatory disease (adenomyosis), or viral infections, since these pathologies may affect the abundance of proteins in serum exosome analysis.
2.2. Serum Sample Collection and EV Isolation
Serum was obtained with blood centrifugation at 5000 rcf for 5 min, and was collected and stored at −80 °C. In order to improve the proteomic study, 100 µL of crude serum was incubated for 5 min with the Albumin Depletion Kit (Thermo Fisher, Waltham, MA, USA). After column elution, EVs were isolated with the Total Exosome Isolation kit (Thermo Fisher Scientific), as reported in [
20]. Then, 100 µL of depleted serum was mixed with 20 µL reagent and incubated for 30 min at 4 °C. After incubation, the samples were centrifuged at 10,000 rcf for 10 min at room temperature, and resuspended with 30 µL of PBS. Sample characterization was performed, as previously reported in [
18]. Protein content was determined using Bradford reagent.
2.3. Exosome Digestion and MS Analysis
An amount of 100 µg of depleted exosomes was digested with the EasyPep™ MS Sample Prep Kits (Thermo Fisher). After digestion, analysis was performed with nanoflow ultra-high performance liquid chromatography high-resolution mass spectrometry, using an Ultimate 3000 nanoLC (Thermo Fisher Scientific, Bremen, Germany) coupled to an Orbitrap Lumos tribrid mass spectrometer (Thermo Fisher Scientific) that used a nanoelectrospray ion source (Thermo Fisher Scientific). A volume of 1 μL of digestion was initially trapped on a PepMap trap column for 1.50 min at a flow rate of 30 μL/min (Thermo Fisher), and then peptides were loaded and separated onto a C18-reversed phase column (250 mm × 75 μm I.D, 2.6 µm, 100 Å, BioZen Phenomenex, Bologna, Italy). The flow rate was set to 300 nL/min. The obile phases were A): 0.1% HCOOH in water v/v, and B): 0.1% HCOOH in ACN/Water v/v 80/20. A linear 60 min gradient was performed. The samples were run in duplicate. HRMS analysis was performed in data-dependent acquisition (DDA), with an MS1 range of 375–1500 m/z; HCD fragmentation was used with normalized collision energy setting 27. Resolution was set at 120,000 for MS1 and 15,000 for MS/MS. Single and unassigned charges were excluded. Quadrupole isolation was set to 3Da. The maximum ion injection times for MS (OT) and the MS/MS (OT) scans were set to auto and to 60 ms, respectively, and ACG values were set to standard. The dynamic exclusion was 30 s. For data processing, raw MS data were analyzed using the Mascot Distiller 2.8 with the Mascot search engine. The MS/MS scans were matched against the human proteome (Uniprot 03/2022 version). The following parameters were used: enzyme trypsin, missed cleavages max 1, mass accuracy tolerance 10 ppm and 0.6 Da for precursors and fragments, respectively. Carbamidomethylcysteine was used as fixed modification, while methionine oxidation as variable. Proteins were considered identified with at least one unique peptide setting a false discovery threshold of <1%. The label-free quantification was performed with Mascot Distiller software, based on the Replicate protocol. This workflow was based on the relative intensities of high-resolution extracted ion chromatograms (XICs) for precursor ions in multiple data sets, and aligned using mass and elution time. Relative quantitation was based on protein ratio calculation, which uses the median of the assigned peptide ratios. The minimum precursor charge was set to 2, and the minimum peptides number was set to 2. The Replicate protocol was used to measure the relative abundance of a protein from sample to sample.
2.4. Western Blotting
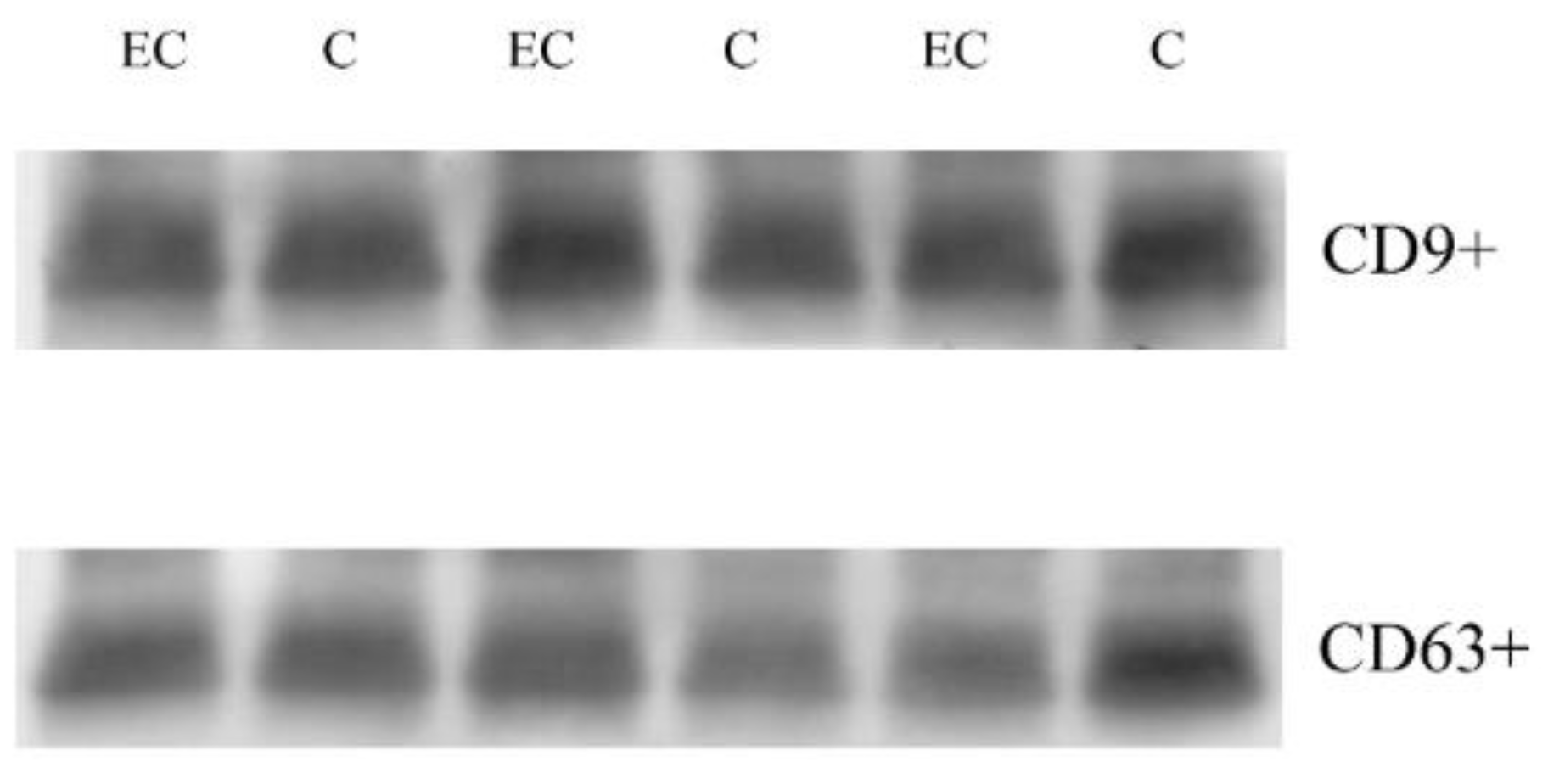
Western blotting in serum exosomes was performed, as previously described [
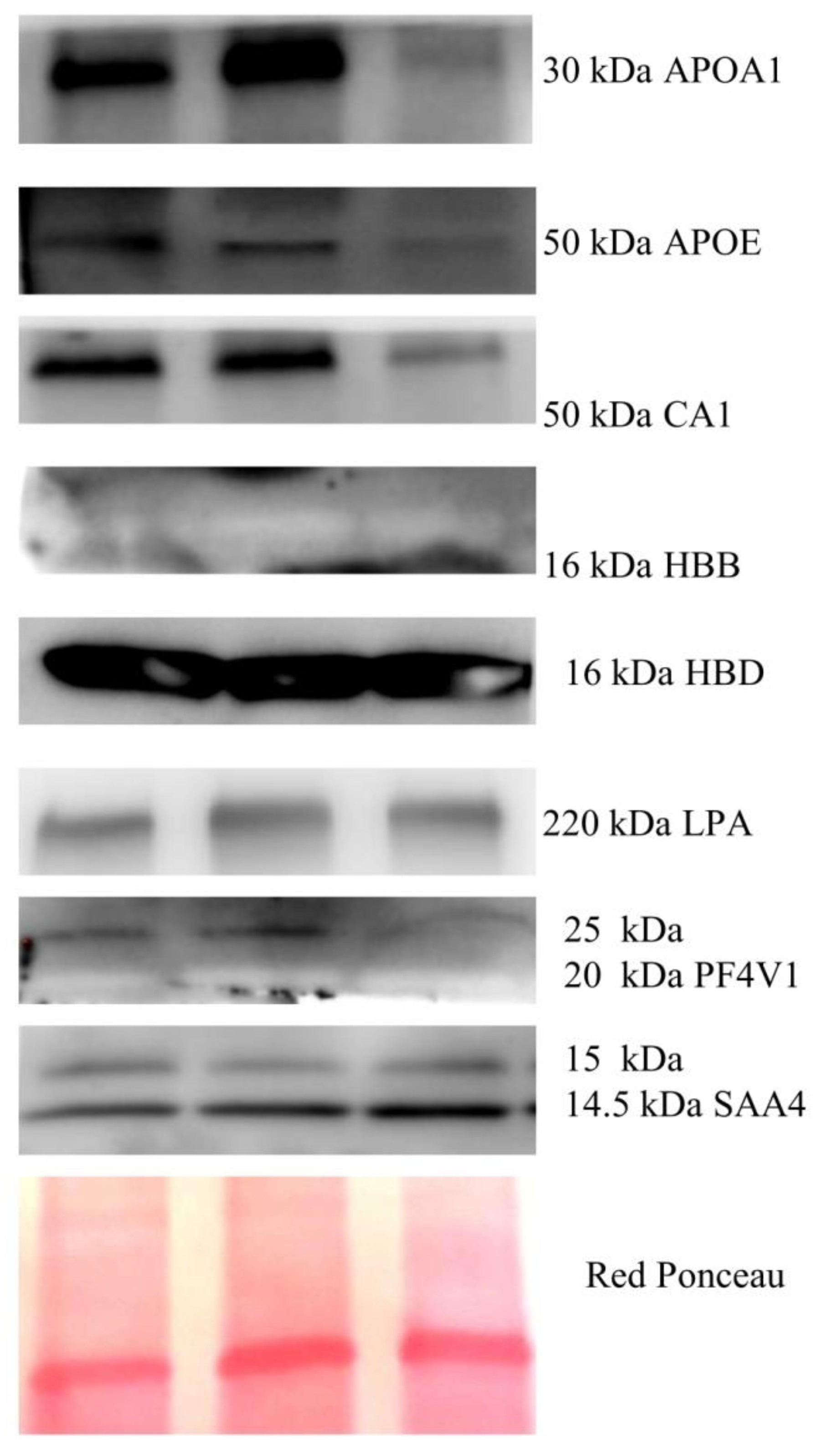
25]. For this analysis, 30 µg of proteins were loaded on precast gel 4–20%, and then transferred to a nitrocellulose membrane; then, the membrane was blocked with 5% defatted milk in TBS-Tween 20 and incubated overnight at 4 °C, with antibodies against CD9 (1:800, rabbit polyclonal), CD64 (1:1000, rabbit polyclonal), LPA (1:800, rabbit polyclonal), PF4V1 (1:2000, rabbit polyclonal), HBD (1:1200, rabbit polyclonal), SAA4 (1:300, rabbit polyclonal), HBB (1:300 mouse monoclonal), CA1 (1:800, rabbit polyclonal), APOE (1:800, rabbit polyclonal), and APOA1 (1:800, rabbit polyclonal). After incubation with primary antibodies, the membranes were incubated with secondary antibodies HRP-conjugated anti-rabbit IgG or anti-mouse IgG (1:3000, Sigma-Aldrich, St. Louis, MO, USA; Merck KGaA, Darmstadt, Germany). The presence of the same proteins was confirmed in the cancer tissue. Western blotting was performed in 30 µg of total lysates from 3 tumor tissues. Tissues were lysed in 1% NP-40, 50 mM Tris-HCl (pH 8.0), NaCl 150 mM with Phosphatase Inhibitor Cocktail Set II 1× (Millipore, Burlington, VT, USA) and 2 mM phenylmethylsulfonyl fluoride (PMSF), and 1 mM benzamidine.
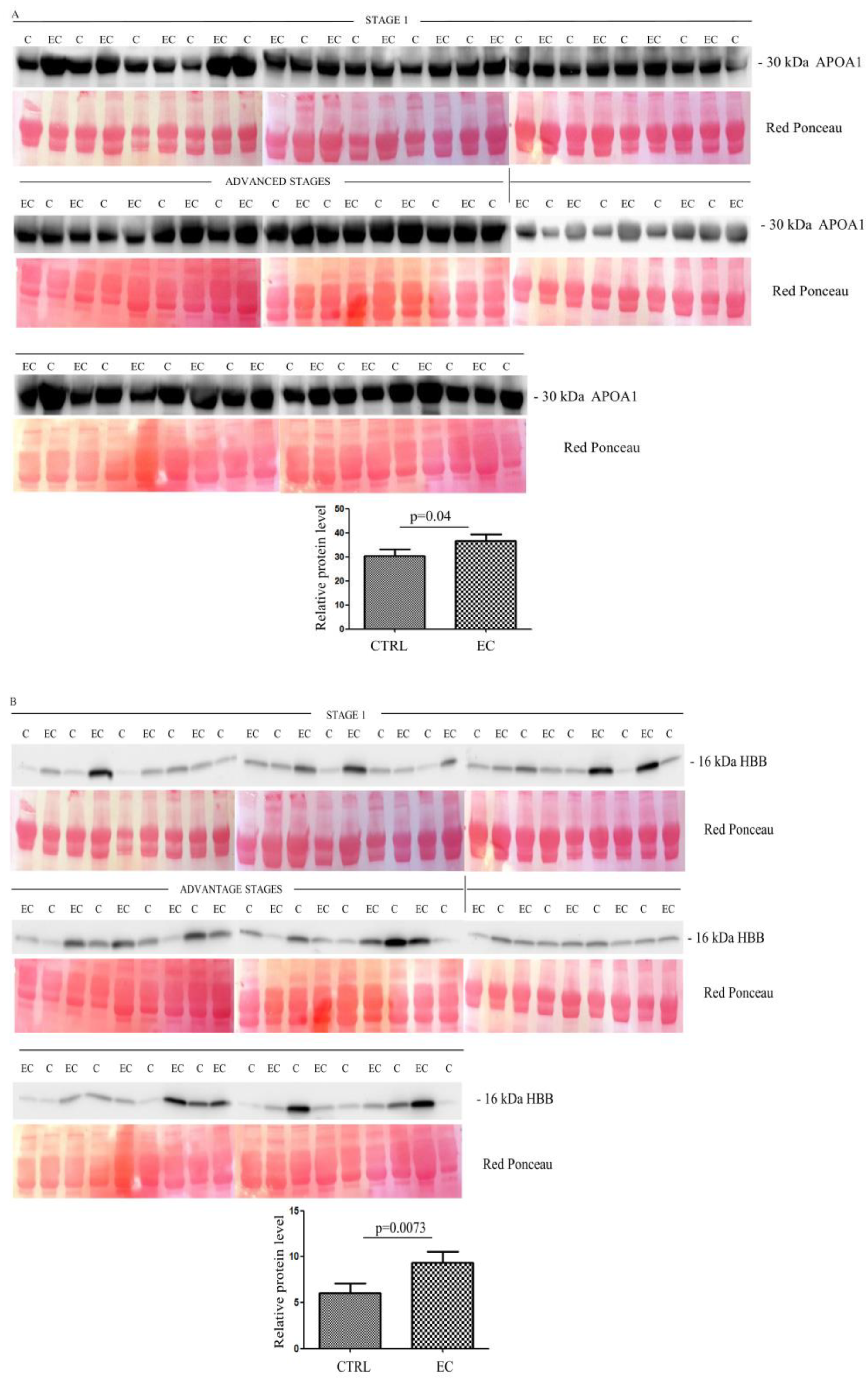
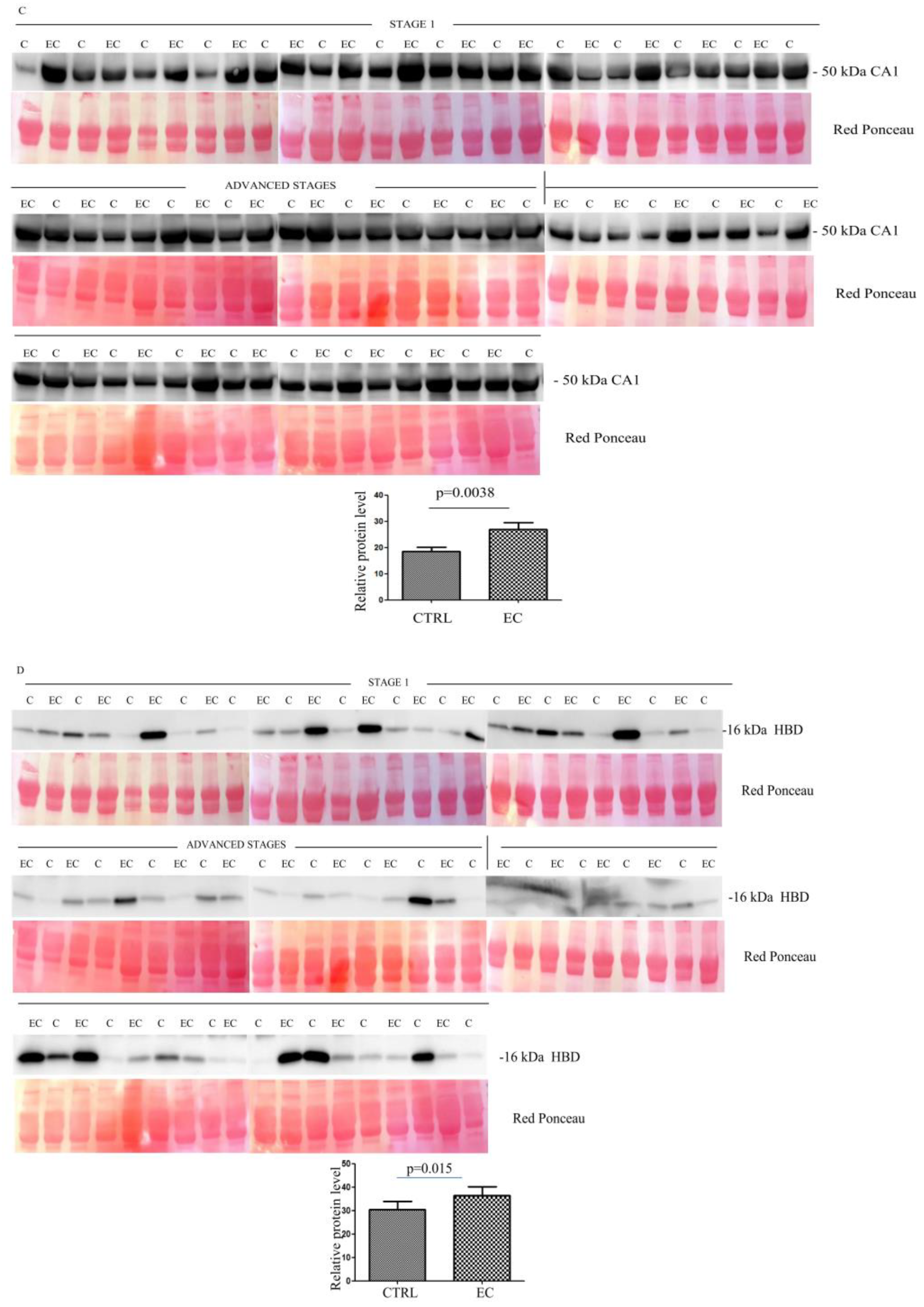
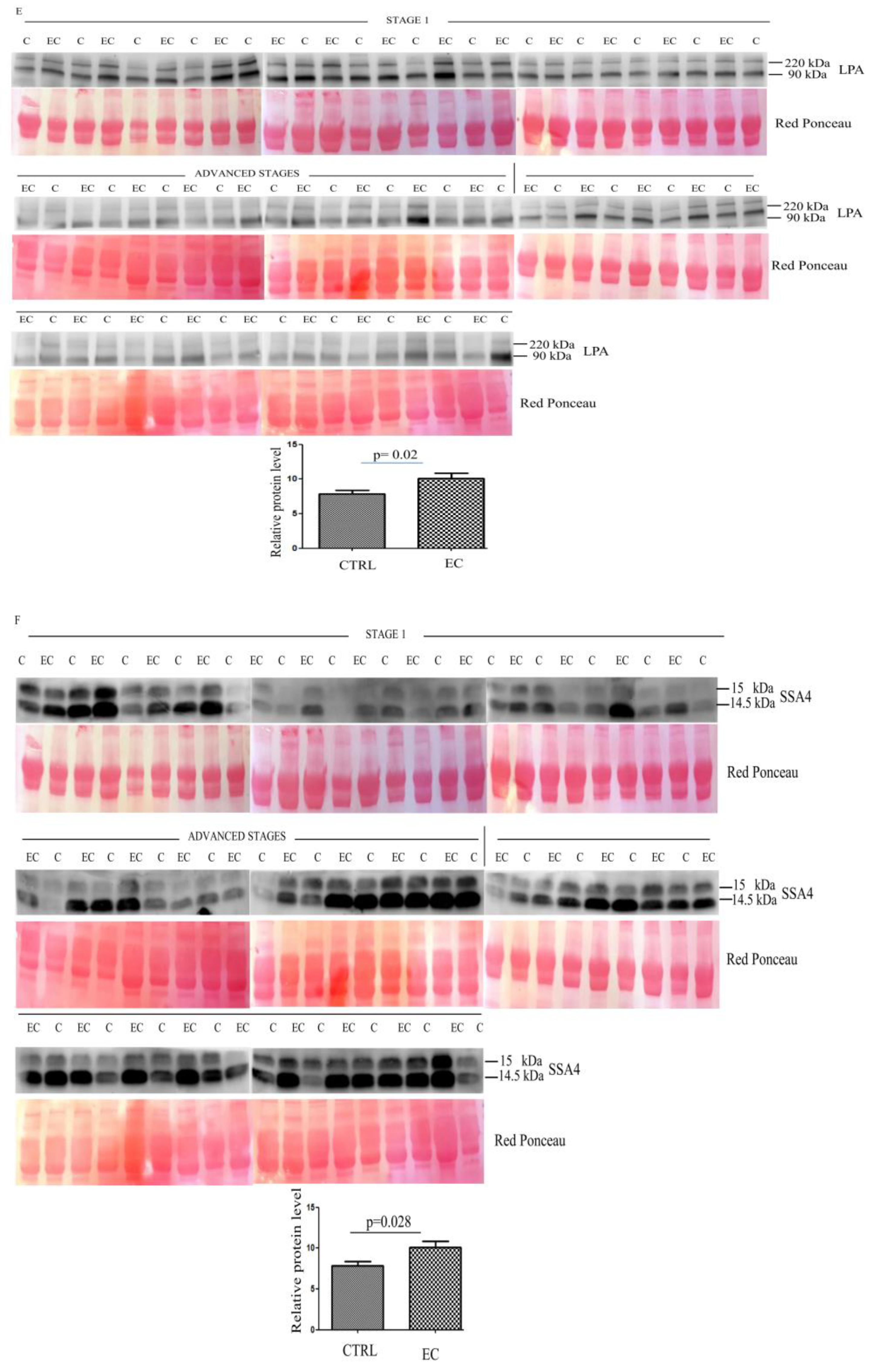
SuperSignal West Pico Chemiluminescent was used for protein band signal visualization. The intensity of the immunostained bands was quantified, normalizing on the total protein content evaluated by the red ponceau solution staining of the membrane from the same blot.
2.5. Bioinformatic Analysis
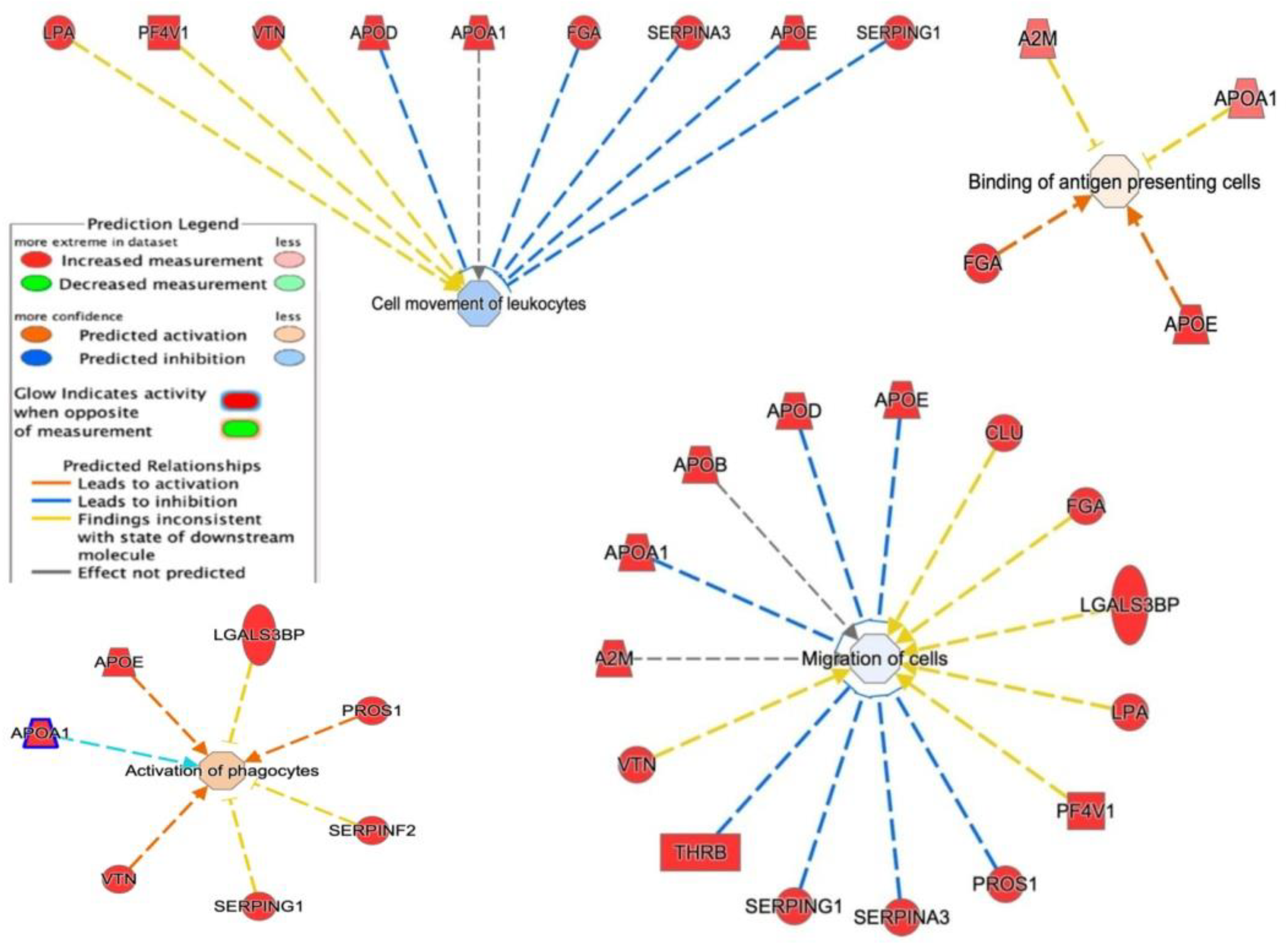
Proteins identified through MS were analyzed with gProfiler classification systems, and categorized according to their molecular function involvement, biological processes, and protein class. Pathway analysis was carried out using the Reactome tool. The bio-functions were generated via Ingenuity Pathway Analysis (IPA) [
26]. Results from the IPA were considered statistically significant when
p < 0.01. For the filter summary, we only considered associations where the confidence was high (predicted), or those that had been observed experimentally.
2.6. Statistical Analysis
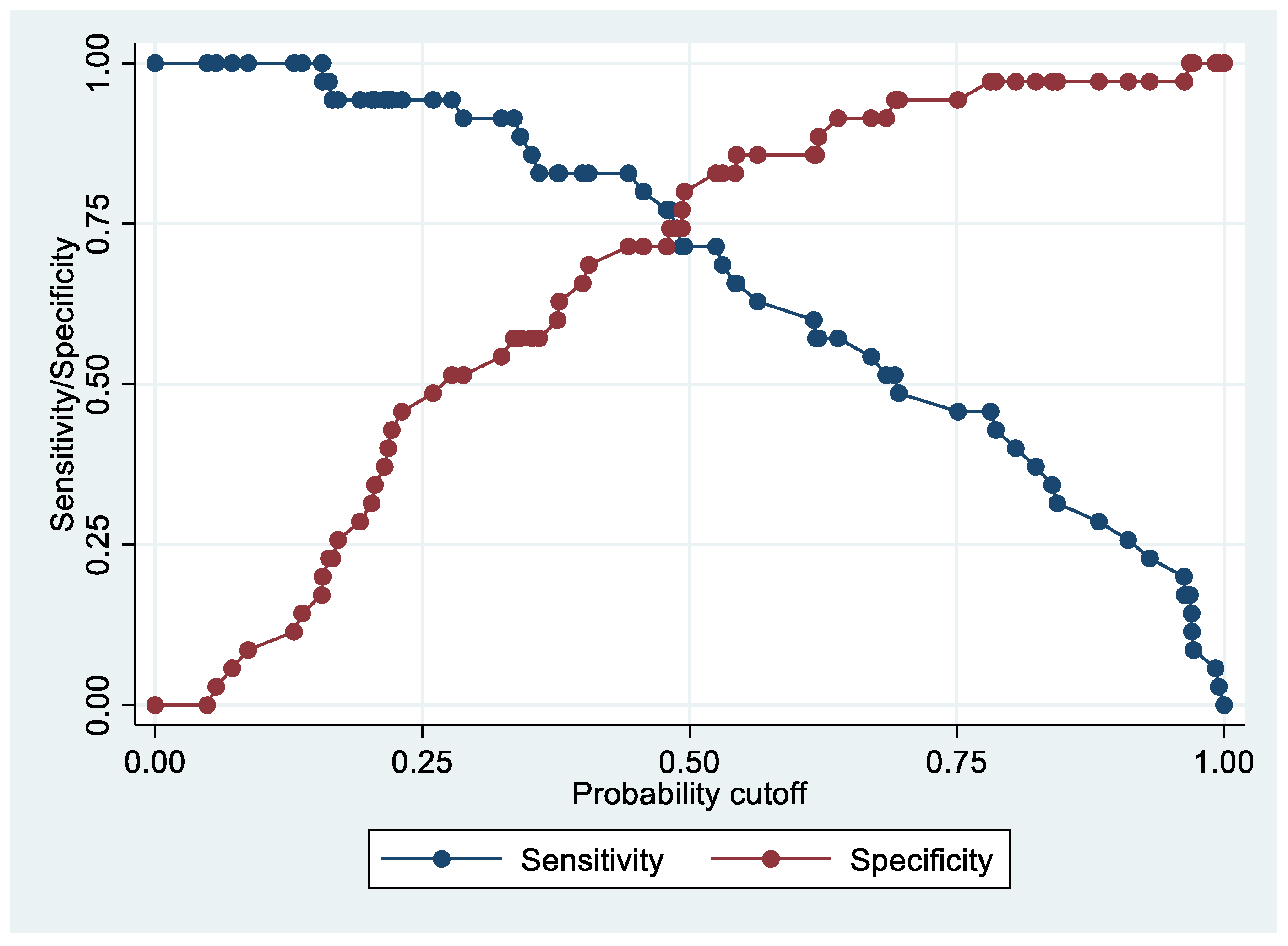
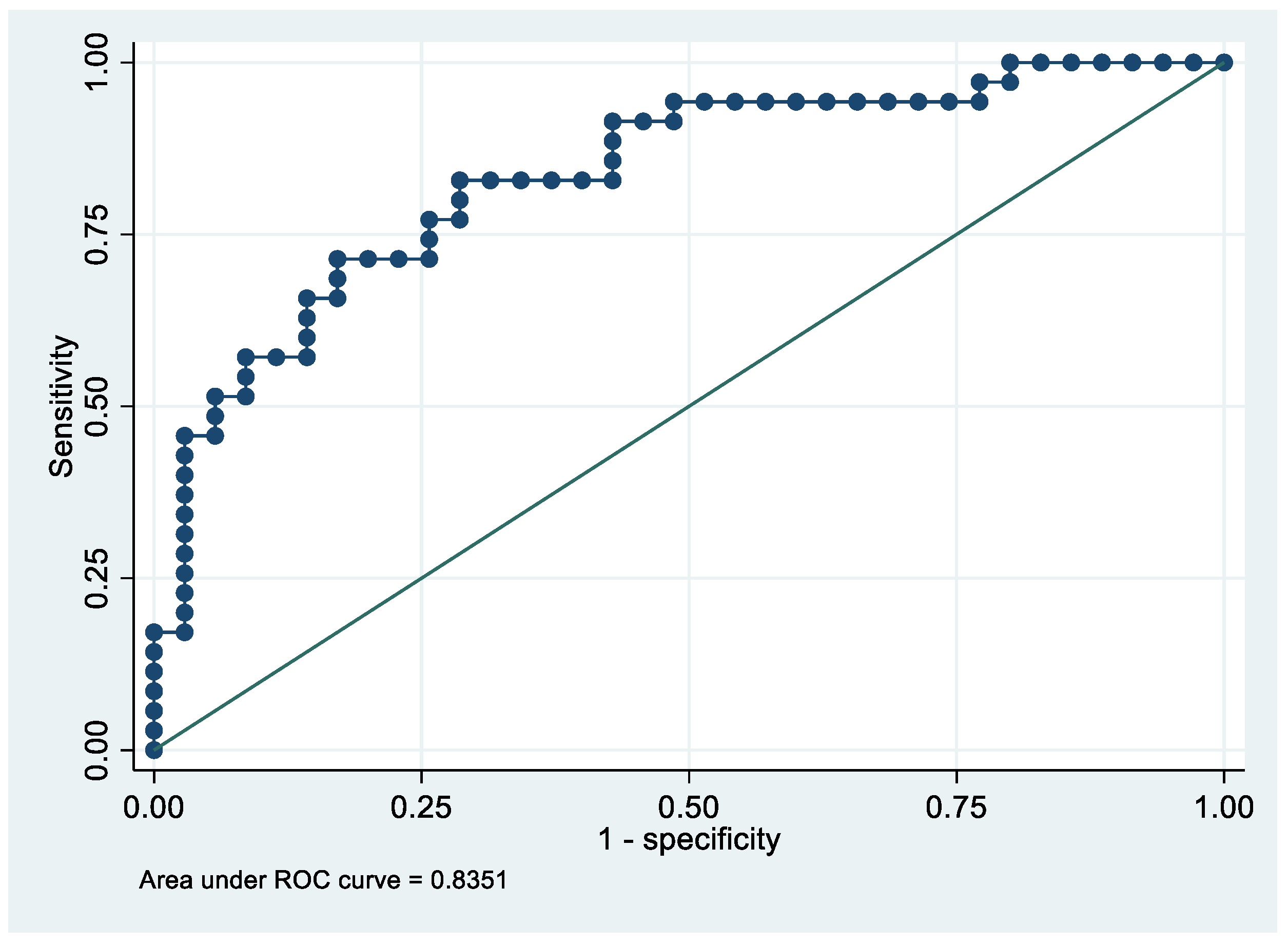
Differences were considered significant between patients and controls when proteins showed a fold change of ±1.5, and satisfied the Mann–Whitney rank sum test (p < 0.05). All analyses were conducted with Stata/IC 16.1 for Windows (StataCorp LP, College Station, TX, USA). Proteins with a fold change ≥ 3.5 and p < 0.05 were further validated. With this selected number of proteins, we elaborated a predictive model using a multivariate logistic regression approach. The dependent variable was EC patients vs. controls. Independent variables were the exosomes selected as explained above. We adopted a step-down procedure, and thus began with all proteins and excluded, one at a time, those which had the highest p-values if p ≥ 0.05. Consequently, the resulting model comprised only exosomal proteins that were significantly associated with the outcome. For this final model, we reported the coefficients of the predictive probability function, the Area under the Receiver Operating Characteristic (ROC) curve (AUC), and levels of sensitivity and specificity. Finally, given that the results of the EC patients vs. controls model were not fully satisfactory, we elaborated two different models using the same multivariate logistic regression, but considered stage 1 EC patients vs. controls and advanced stage (2, 3, and 4) EC patients vs. controls separately.
4. Discussion
Cancer biomarkers help to characterize tumor alterations, and are frequently used for the diagnosis and prognosis of the disease, and for determination of a personalized treatment [
27]. Exosomes are microvesicles that, once released, play key roles in tumor growth and invasion. The proteomic characterization of patients’ exosomes is still challenging, but may represent a key step in the discovery of new potential biomarkers, particularly at an early stage [
28]. LC-MS/MS has been successfully used to identify the proteomic profile of exosomes, and for biomarker identification as in prostate cancer [
29], bladder cancer [
30], and ovarian cancer serum [
31]. In EC, thanks to proteomic approaches (such as two-dimensional electrophoresis, protein arrays, and mass spectrometry), hundreds of proteins have been reported as potential biomarkers in cancer tissue, blood, its derivatives, and other body fluids (17,18). Nevertheless, none of them have reached clinical stages, probably due to lack of tissue specificity, and also since most of them are proteins that are involved in broad processes including metabolic pathways, inflammatory responses, cell adhesion, and in hormones. To find specific non-invasive biomarkers, there is growing interest in exploring exosome-enriched proteins.
Interestingly, Song et al. recently found that plasma exosomes from EC patients are enriched in LGALS3BP, a protein that also promotes endometrial cancer progression.
In this study, we used a larger cohort of EC patients to identify novel exosomal biomarkers, and investigated the exosome proteome from albumin-depleted serum, using LFQ based proteomics followed by Western blotting analysis validation.
Starting with the proteomic profile, we obtained 440 proteins that were further selected based on the strongest differences in abundances; then, we applied a multivariate logistic regression analysis for all EC stages (1, 2, 3, and 4). By this analysis, we found that PF4V1, APOE, and HBD allowed us to separate cases from controls with an AUC = 83.5% in 36 EC patients as compared to 36 healthy individuals.
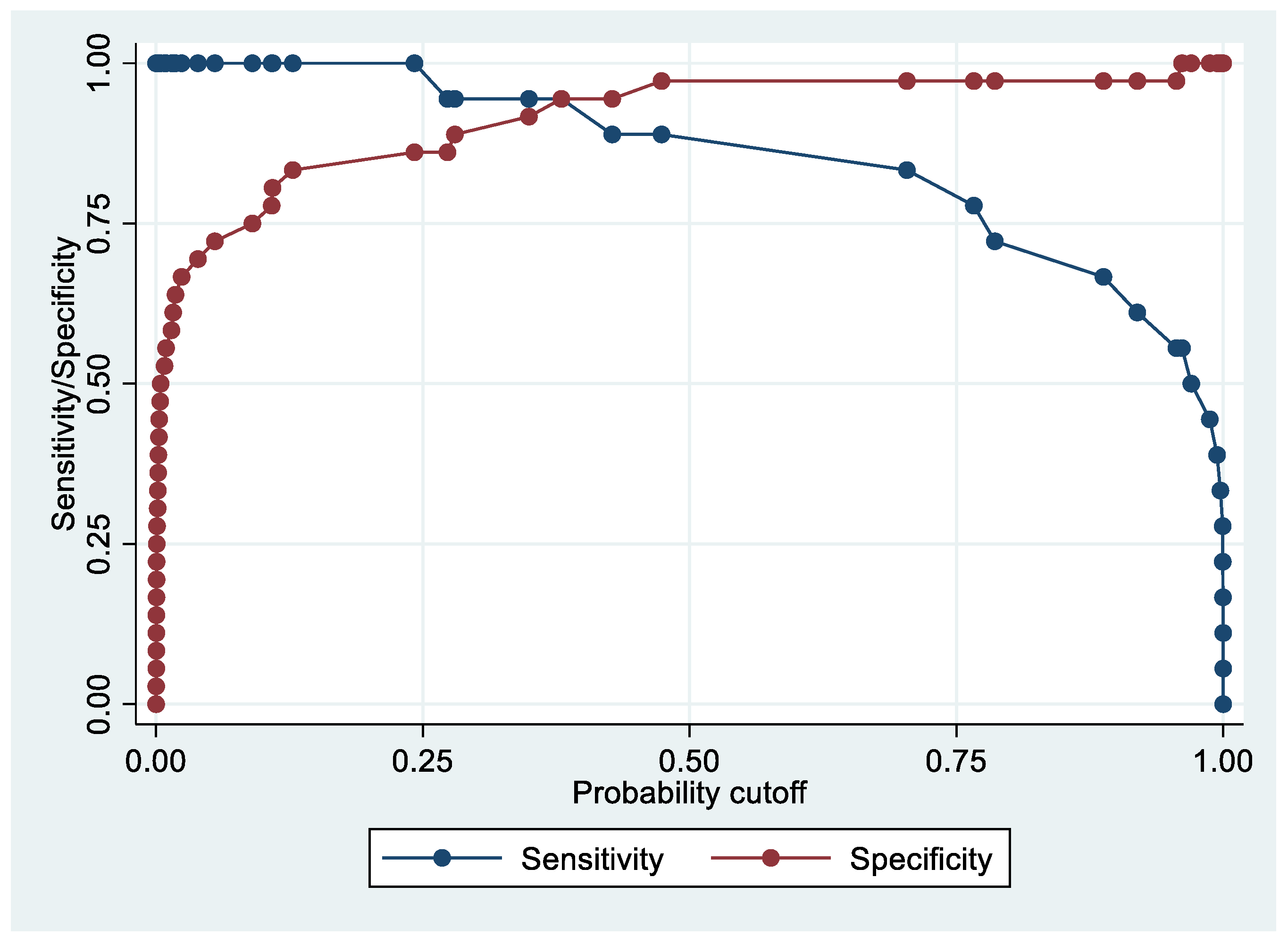
Considering that this result was not fully satisfactory, and attempting to find early EC biomarkers, we decided to separate patients into stage 1 (often asymptomatic patients) and advanced stages (2, 3, and 4).
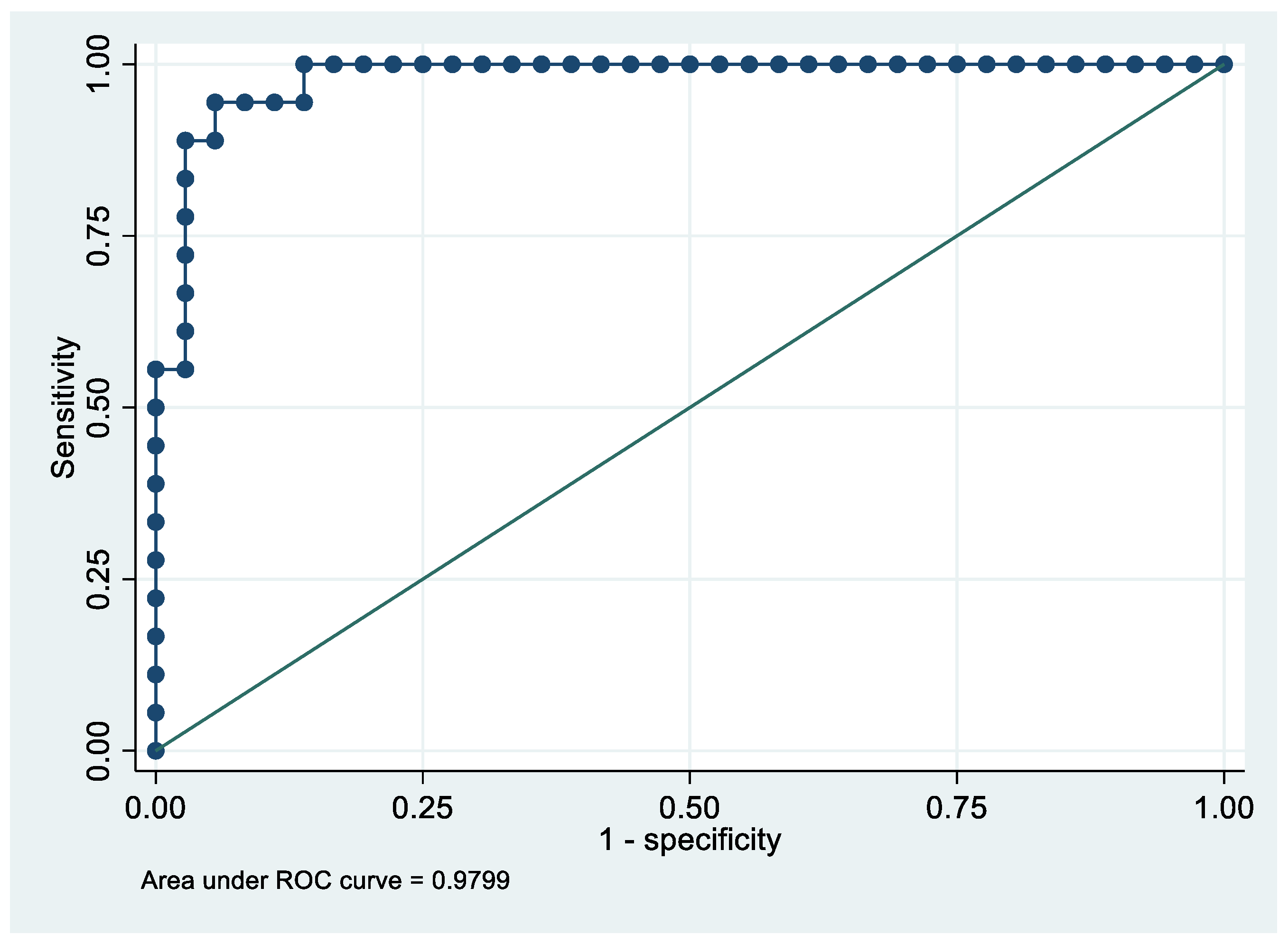
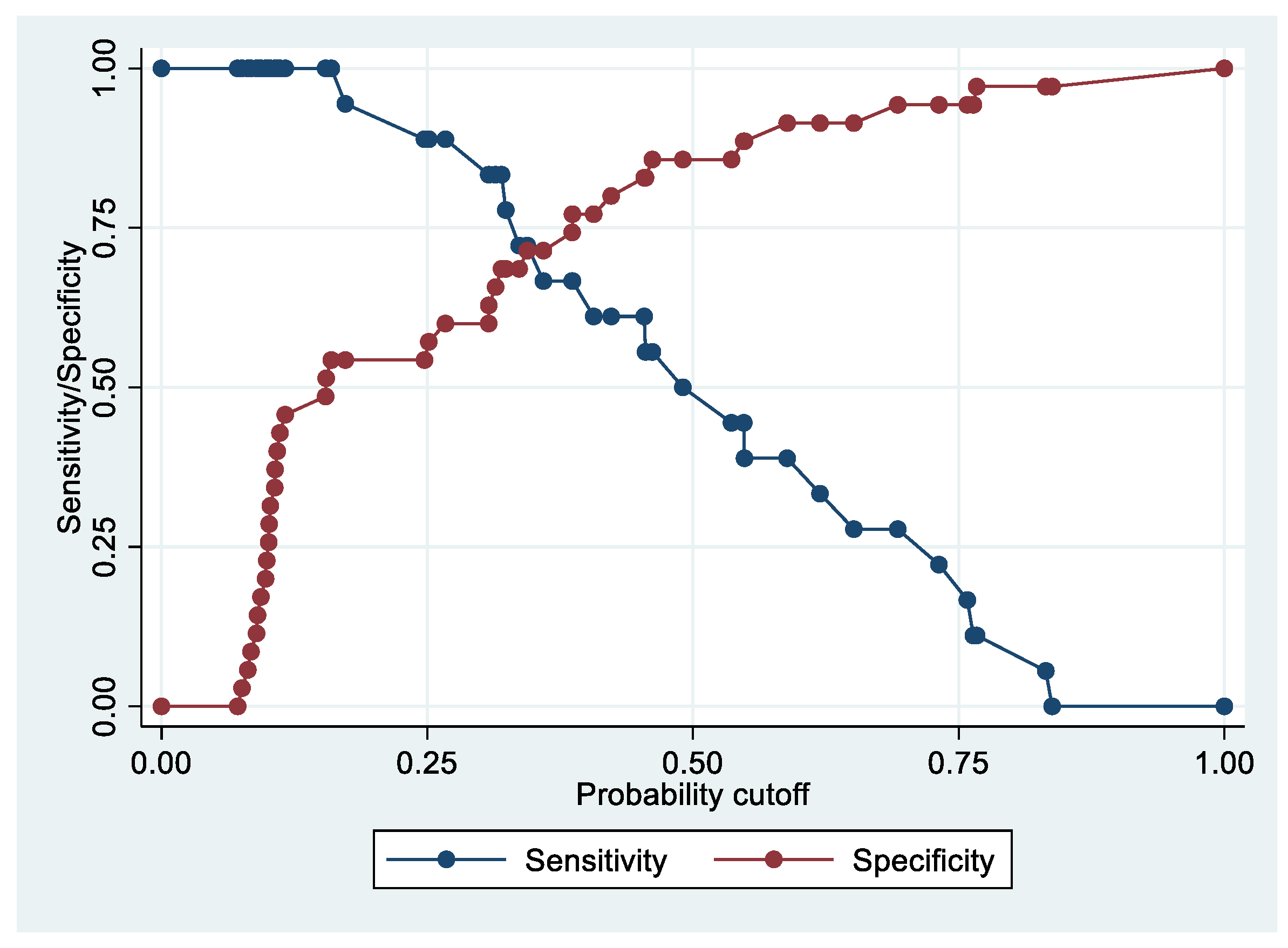
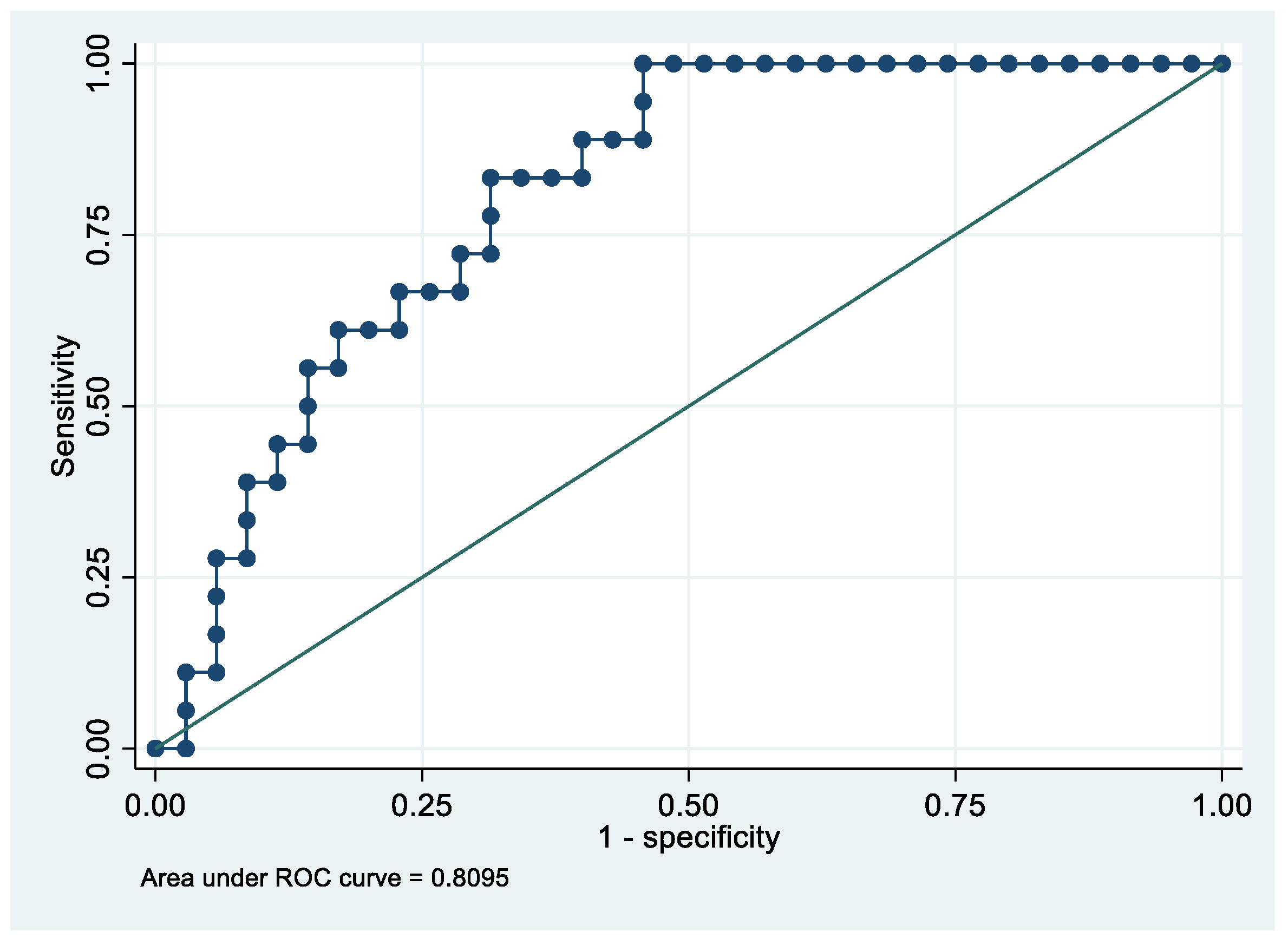
A multivariate logistic regression model for stage 1 (18 patients) based on PF4V1, CA1, and HBD allowed us to separate cases from controls with an AUC = 98.0%. The last multivariate logistic regression model was performed that compared patients with an advanced stage EC (2, 3, or 4) (18 patients). Based on ApoE expression, it allowed us to separate cases from controls with an AUC = 80.9%. The best and only fully satisfactory model was that of the analysis that considered stage 1 patients. It is noteworthy that proteins that discriminate stage 1 ECs well do not satisfactorily discriminate all stages of EC. The low performance of these proteins in the more advanced stages of the disease is interesting, and requires further investigation. This study shows that stage 1 discriminating proteins do not work well for more advanced stages of EC.
Reactome analysis revealed that EC exosome proteins are involved in dysregulation of plasma lipoprotein assembly and remodeling, hemostasis, and platelet degranulation pathways that may be involved in cancer development.
CA1 is a member of the carbonic anhydrase (CA) family, and an overexpression in osteosarcoma cells leads to calcification with ascorbic acid [
32]. Wang et al., in a proteomic study, identified this protein in stage I non-small cell lung cancer, and validated its overexpression via Western blotting; this represents a promising early biomarker for non-small cell lung cancer.
HBB is involved in oxygen transport from the lung to several peripheral tissues [
33]. Expression of HBB in lung cancer cells and breast cancer cells is associated with ROS cytotoxicity suppression, leading to cancer cell survival and spread [
34].
PF4V1 suppresses chemokine angiogenesis by blocking the protein bFGF, and is closely associated with the growth and metastasis of various cancers [
35]. It is known that PF4V1 in prostate cancer leads to suppression of proliferation and invasion, and serves as a potential prognostic biomarker [
36].
APOE is a protein associated with lipid particles, that mainly functions in lipoprotein-mediated lipid transport between organs via the plasma and interstitial fluid [
37]. Studies on several tumors, including glioblastoma [
38], EC [
39], lung cancer [
40], and prostate cancer [
41], showed that when APOE is overexpressed, the disease is more aggressive, and the prognosis is poor [
42].
Of note, although these proteins are commonly found in plasma upon liver secretion, in this study we found that they are detectable in endometrial tumor tissue; thus, they may represent bona fide EC biomarkers when secreted into exosomes by tumor cells.
Interestingly, through Western blotting we noticed that CA1, PF4V1, and APOE displayed higher molecular weights than the canonical ones. This may rely on the glycosylation of proteins in exosomes, as previously described by the literature [
43]. Whether glycosylation may affect protein functions or exosome distribution is still unknown, and is of great interest.
Importantly, in this study we provided a proteomic profile of EC serum exosomes that suggests new promising non-invasive biomarkers, although we are aware of some limitations. These proteins have not yielded satisfactory results for all stages together, or for the more advanced stages of EC. However, in the discovery phase, we identified proteins that discriminated well between controls and stage 1 patients. This suggests that for advanced stages, separate studies are needed, as biomarkers that work well for stage 1 are not necessarily efficient for advanced stages or all stages together. Moreover, we are aware that broader studies are needed to validate the role of the identified proteins in larger cohorts of patients. Another weakness of our study is that patients of the discovery phase were also included in the validation phase, which, however, was performed in a larger cohort that included 24 patients that did not overlap with the previous ones. Lastly, since levels of some proteins may change with age, we think that validating these results with age-matched cases and controls should be the next step to ascertain the potential of these proteins as biomarkers.


 ,
, 
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}